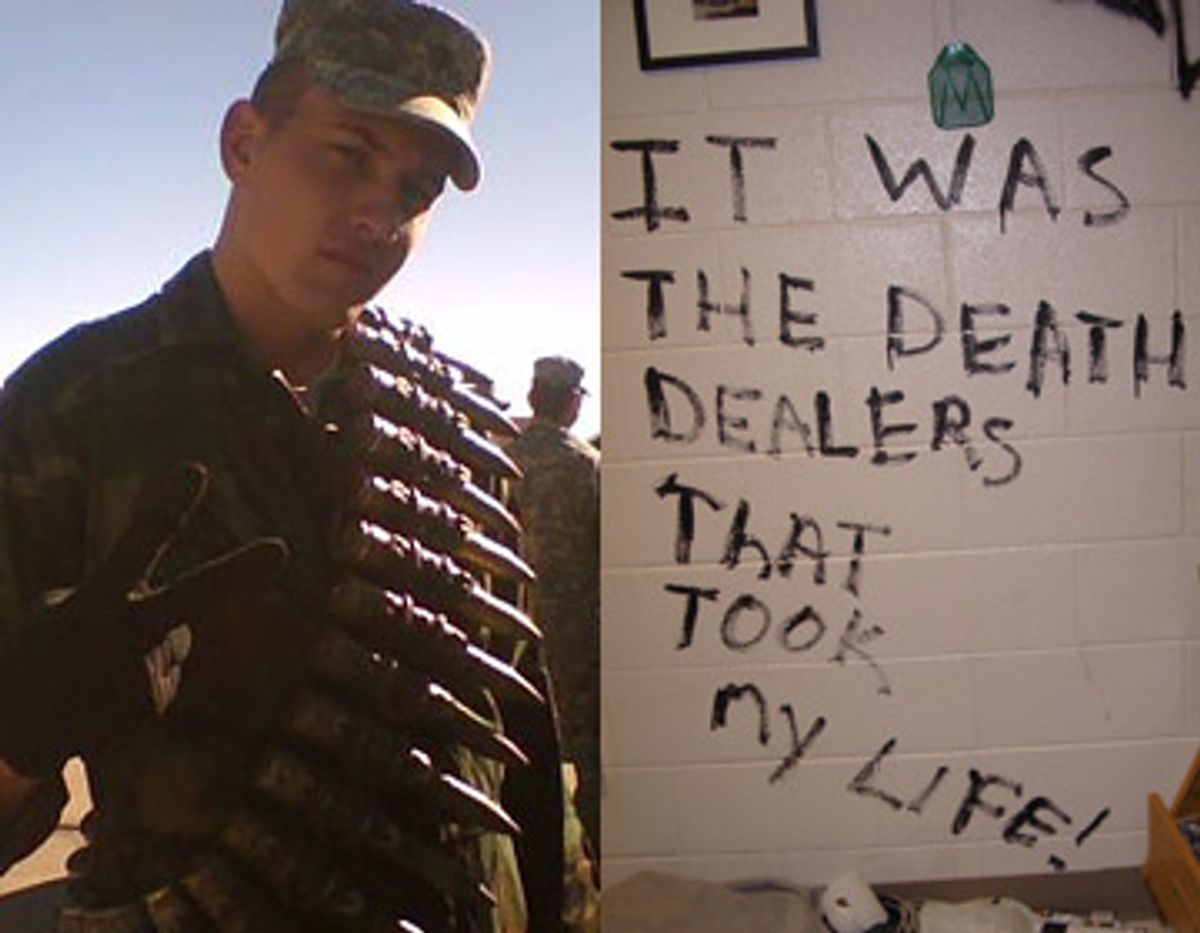
The day before Halloween 2008, Army Pvt. Adam Lieberman swallowed handfuls of prescription pain pills and psychotropic drugs. Then he picked up a can of black paint and smeared onto the wall of his room in the Fort Carson barracks what he thought would be his last words to the world.
"I FACED THE ENEMY AND LIVED!" Lieberman painted on the wall in big, black letters. "IT WAS THE DEATH DEALERS THAT TOOK MY LIFE!"
Soldiers called Lieberman's unit, the 1st Battalion, 67th Armored Regiment, the Death Dealers. Adam suffered serious mental health problems after a year of combat in Iraq. The Army, however, blamed his problems on a personality disorder, anxiety disorder or alcohol abuse -- anything but the war. Instead of receiving treatment from the Army for his war-related problems, Adam faced something more akin to harassment. He was punished and demoted for his bad behavior, but not treated effectively for its cause. The Army's fervent tough-guy atmosphere discouraged Adam from seeking help. Eventually he saw no other way out. Now, in what was to be his last message, he pointed the finger at the Army for his death.
It would be a voice from beyond the grave, he thought, screaming in uppercase letters. The last words, "THAT TOOK MY LIFE!" tilted down the wall in a slur, as the concoction of drugs seeped into Adam's brain.
Late last month the Army released figures showing the highest suicide rate among soldiers in three decades. The Army says 128 soldiers committed suicide in 2008 with another 15 still under investigation. "Why do the numbers keep going up?" Army Secretary Pete Geren said at a Pentagon news conference Jan. 29. "We can't tell you." The Army announced a $50 million study to figure it out.
It is not just the suicides spiraling out of control. Salon assembled a sample of 25 cases of suicide, prescription drug overdoses or murder involving Fort Carson soldiers over the past four years, by no means a comprehensive list. In-depth study of 10 of those cases revealed a pattern of preventable deaths. In most cases, the deaths seemed avoidable if the Army had better handled garden-variety combat stress reactions.
Interviews, Army documents and medical records suggest that Adam might not have attempted suicide if he had received a proper diagnosis and treatment. His suicide attempt seems avoidable. But the Army's mistreatment extended well into its aftermath.
- - - - - - - - - - - -
At the last minute on Oct. 30, Lieberman stumbled out of his room and dialed 911. He lived.
Five days later Adam's mother, Heidi Lieberman, sat opposite the desk of Lieberman's battalion commander, Lt. Col. Lance Kohler, at Fort Carson. Nobody from the Army had bothered to call her in Rochester, N.Y., to tell her about Adam's suicide attempt. There was no requirement to alert parents of an attempt, the Army said, only a successful suicide.
Heidi had watched her son's mental health deteriorate precipitously after he returned from Iraq in late 2006. He had suffered from a laundry list of symptoms typical of post-traumatic stress disorder, including insomnia, depression, panic attacks and flashes of violent anger.
Two days after he swallowed the pills, Adam called his mother himself from the hospital. With her son still slurring his words from the effect of the meds, Heidi could barely understand him. When Heidi asked him where he was, Adam had to ask someone.
Sitting across from the lieutenant colonel's desk, Heidi wanted to know why the Army had not moved her son into a unit supposedly dedicated to healthcare where he might get better treatment.
"Well, he has legals," Kohler told her. Legal trouble. She knew Adam was struggling. Mostly Adam had been silencing his demons with 30 beers a day plus some Jameson. He'd puke in a bucket and start over. Mental health professionals call it self-medicating when a soldier comes back from war and turns to booze when he can't get help, another typical reaction. Just as predictable is the bad behavior that comes with it.
To Heidi, Kohler's response showed that the Army considered Adam a discipline problem, but didn't seem particularly concerned about why.
"What legals?" Heidi asked.
Adam had broken into a candy machine, so petty larceny. He had also gone AWOL for a short time to say goodbye to an Army buddy in Texas headed off to a second tour in Iraq. The Army denied Adam's request for leave. He went anyway.
"And defacing government property," Kohler added to the list.
"When did he do this?"
"Within the last couple of days," Kohler responded, staring.
Heidi thought. No. Couldn't be.
"What did he deface?"
Kohler stared. "The wall in his bedroom."
Heidi met his stare, exasperated. "You mean his suicide note?" Kohler just looked at her.
The next day Heidi called Adam's company commander, Capt. Phelps.
"You know," Heidi fired at Phelps, "I still have a hard time wrapping my mind around the fact that my son is being charged with defacing government property and you people are more concerned about your wall than my son," she stammered. Then she threatened, half jokingly, "I will paint that wall and make this stupidity go away."
A pause, and then Phelps snapped, "We'll contact supply and have them bring you the matching paint."
And so, the Army allowed a mother to paint over her son's suicide note. Heidi's handicapped sister helped.
"I was kind of surprised that they took me up on that," she said late last year sitting at her dining room table in her home in Rochester, N.Y. Heidi's sister took photos of her, paint roller in hand, erasing what was supposed to be her son's last message. "He agreed that if I painted that wall that charge would go away," she recalled about her talk with Adam's captain. "It didn't."
Just before Christmas, MPs fingerprinted and booked Adam for defacing government property.
- - - - - - - - - - - -
A blondish crew cut tops Adam Lieberman's lanky, lumbering 6-foot-6 frame. He makes little eye contact. Adam joined the Army at age 17. In late 2005 he deployed to Iraq with the 4th Infantry Division as a forward observer, a radioman. He is all of 21 now.
More than two years after his return from Iraq, where several close explosions rocked his skull, his memory sometimes fails him. He carries a notebook to keep track of appointments. He still writes the occasional letter backward.
Adam is now at the stage of digesting (or at least sharing) his experiences in Iraq in a passive tense -- he describes things happening to him and around him, rather than by him. He arrived at the scene of a roadside bomb attack on other U.S. troops in Sadr City in Baghdad. "A guy's face was blown off from his nose to his chin," he said as we sat at his dining room table with Heidi while he was home on leave recently. The U.S. soldier was gagging, drowning in blood without a mouth or nose. A medic performed an emergency tracheotomy. The soldier died anyway.
Adam didn't even bother to inspect the nearby Humvee that took a direct hit. He could see through the windows that inside the vehicle, "It was blood soup."
During another engagement a gunner atop Adam's Humvee suddenly collapsed in Adam's lap. Only a thin flap of skin attached the gunner's head and torso. Beheaded. Adam vomited.
He once saw the lower half of a friend's body sheared off by a roadside bomb. In the seconds that followed before he died, his friend still moved his right arm and tried to talk. He looked at Adam. Adam described the look in his eyes as "terror."
Adam once took a sniper's bullet to the chest. It shattered his digital camera and hit his body armor. On two separate occasions he lost consciousness because of head blows.
Heidi noticed a difference in Adam when she met him at the airport in December 2006. "When he got off the plane and we were walking, I saw his eyes shifting through the crowd," she remembered.
Crowds freaked him out. Adam had a panic attack in a Wal-Mart. He started getting into fights at bars. He couldn't sleep. "You become a new person," he explained. "You are raised as a person and they send us over there and we become a new person."
The Army "screened" Adam for mental health problems upon his return from Iraq, a process Adam describes as, "You stand in a line and go to a bunch of tables where people are sitting." He filled out some forms. Some soldiers aren't yet aware of their problems at that point. Some lie because they just want to go home with their wives. Others say they report problems but receive little follow-up.
"Nobody is willing to help anybody," he said about his experience at Fort Carson after returning from Iraq. "You have to understand. We are just pieces of equipment."
The Army says it is working hard to erase the stigma of seeking mental healthcare. It isn't working at Fort Carson. Adam says he was actively discouraged from looking for help.
"If you have a problem, you are going to be a problem," he explained. "You don't ask for help -- ever. That is just the Army's way. Always will be."
A document obtained from another unit at Fort Carson supports Adam's description of a culture that discourages "weakness." Someone in the 3rd Brigade Combat Team prepared a mock official form called a "Hurt Feelings Report," and left a stack of copies near a sheet where soldiers sign out to see a doctor. (View it here.)
"Reasons for filing this report: Please circle Yes or No," the Hurt Feelings Report directs. Options include: I am thin skinned; I am a pussy; I have woman-like hormones; I am a queer; I am a little bitch; I am a cry baby; I want my mommy; All of the above. A blank appears after, "Name of 'Real Man' who hurt your sensitive feelings."
Maj. Gen. Mark Graham, the Fort Carson commander, admits that the attitude of Army personnel toward mental healthcare needs work. "Because of the focus we have had on behavioral health, we have seen an increase in soldiers coming forward to get help," he told me. "Is it as many as we think are out there? No, it is not. Do I think that we still have a stigma challenge here? Absolutely, we do."
By December of 2007, Adam was getting increasingly violent. "I fucking punched a guy," he recalled about a fight in the barracks. "I dragged him out of my room and threw him down the stairs." On Dec. 20, 2007, he filled out an Army "PTSD checklist." He checked off being "extremely bothered" by flashbacks, nightmares, bad memories, emotional numbness, insomnia and angry outbursts. He also reported panic attacks and jumpiness, among other things.
Col. Elspeth Ritchie, the Army's top psychiatrist, ticks off a series of initiatives to improve Army mental healthcare, including the hiring of 250 new mental health providers through civilian contracts and more than 40 marriage and family therapists since the spring of 2007. Ritchie said an August 2007 Army directive ensures PTSD screenings for soldiers with disciplinary problems so serious the Army wants them out. She added that the Army surgeon general issued a memo in May 2008 requiring additional review of any diagnoses short of PTSD to make sure the Army gets it right. "We've really tried to enhance our access to care," she said in a telephone interview.
Though Adam filled out his checklist in late 2007, the initiatives Ritchie describes did not trickle down to him. Throughout this entire period, Adam's medical records show, the Army focused almost completely on his misbehavior, like drinking and fighting, and demoted him from specialist to private, but did not address the root cause. The Army enrolled Adam in an Army substance abuse program he called a "joke." The Army wanted him to work on anger management. "I was like, 'I don't have anger problems. You people are causing me to be angry.'"
By the spring of 2008, Adam's condition had deteriorated. "He called me in April and said he really wanted to die," Heidi recalled. "He told me he had his Mustang up to 120 and pointed at a cliff. I told him he needed to get help now. No more dealing with it on his own."
This time Adam checked himself into a private facility. A doctor soon informed him he had PTSD from his experience in Iraq. "That's when I started figuring it out myself," Adam told me. "I realized I was not an alcoholic, I was just self-medicating."
After a few weeks, however, Adam had to return to Fort Carson, where the Army still basically considered him a drunk and a discipline problem.
That's contrary to proper treatment of PTSD. "The best way to treat it is to identify it appropriately," said Dr. Anthony Ng, a psychiatrist and board member of Mental Health America.
In addition to hundreds of pages of medical records he gave me, Adam agreed to hand over a copy of his illustrated journal. An undated entry from after his private hospitalization notes that, "Since returning from the hospital my ball of twine has been unraveling fast. ... The woman at [Fort Carson's] mental health dismissed me as if I were a bum asking for money," he wrote, and then recorded one of those flashes of anger common to soldiers with PTSD. "I wanted to rip her jaw off and scrape the skin off her face with her Goddamn teeth."
"But I wasn't surprised," Adam's entry continues. "That's Army health care."
In June or July 2008, he got a call from an Army psychologist. "She didn't even know my name," he told me. "I'd seen her three times. How is she going to help me if she can't even remember my name?"
The Army also seems to have resisted recognizing Adam's likely traumatic brain injury, given his head blows in Iraq and subsequent memory loss and other symptoms. The Army put him through a battery of tests on Oct. 15 to determine if he might be eligible for disability pay for a brain injury. Adam tested "within normal limits," his medical records show. "There is no evidence of clinically significant cognitive impairments."
(Civilian neurosurgeons generally say that doctors should stash the tests and MRI exams for the most part, since TBI is notoriously difficult to pin down that way, and look to behavior instead. Patients with a history of head trauma who present with obvious symptoms should receive swift treatment for TBI).
Adam's Army medical records from Oct. 30, the day of his suicide attempt, look similar to all of his Army medical records. The Army psychologist noted "alcohol dependence with continuous drinking behavior," depression and anxiety disorder -- his problems, not the Army's.
A diagnosis of PTSD from combat would require the Army to pay Adam a lifetime of benefit checks. The Army would not have to pay if a doctor were to find instead that his mental problems were preexisting and/or unrelated to his Army service. Adam said his Army psychologist "has been trying to give me a personality disorder since Day One, that I wanted to kill people before I got into the Army." Soldiers also don't get benefits if they are ushered out the door with dishonorable discharges for misbehaving.
On Oct. 30 the Army psychologist noted "homicidal ideation," or thinking about murder, but "no homicidal plans." She also noted "no suicidal ideation."
Adam admitted he lied on that one. He had made up his mind. "I didn't want her to interfere," he said. "I was thinking about killing myself, but I was restricted to post for drinking on duty so I could not get my gun. I went to my room and swallowed all my pills."
Adam painted his note on the wall. And then he changed his mind. An ambulance rushed him to the hospital. He "remember[s] them trying to get me to drink this charcoal stuff" at the hospital, but not much more. "I woke up and I was chained to the bed."
Nine days after Adam's suicide attempt, the Army psychologist changed her diagnosis, according to Adam's medical records. He had "chronic post-traumatic stress disorder." It was the first time the Army seemed willing to admit that a year of war caused Adam's problems. "It took me trying to kill myself for her to put it on there," Adam told me.
- - - - - - - - - - - -
Unfortunately, the problem likely goes beyond Fort Carson. Maj. Gen. Graham, the Fort Carson commander, makes noted efforts to recognize and address the problems. "Our goal is to get in front of this," Graham said in a telephone interview. "Instead of doing the investigation following a suicide, to find out how this happened and how we could have prevented it, what we want to do is actually prevent them and get in front of this and figure out how you help a soldier before it gets to a point of critical mass and something horrible is going to happen," he added. "Are we perfect? No. Are we trying? We are. Can we do better? Of course we can."
Graham's power to do better is limited, however. The Army Medical Command runs medical care at Fort Carson and other Army posts. MEDCOM reports to the Army surgeon general, Lt. Gen. Eric Schoomaker, not Graham.
And some Army fighting units, or "line" units, stationed at Graham's post have failed to incorporate the prevention, recognition and treatment of combat stress into their wartime mission. At Fort Carson a mental problem from combat is still a scarlet letter.
Meanwhile, the deaths keep coming. At least three Fort Carson soldiers died in apparent suicides in January. (Fort Carson quibbles with this statistic, claiming that one of the three had not completed the paperwork to be officially stationed at Fort Carson. The death of a second soldier, found dead in his home from a "drug interaction," is still under investigation.)
(The second installment in Salon's "Coming Home" series will appear tomorrow.)
Shares